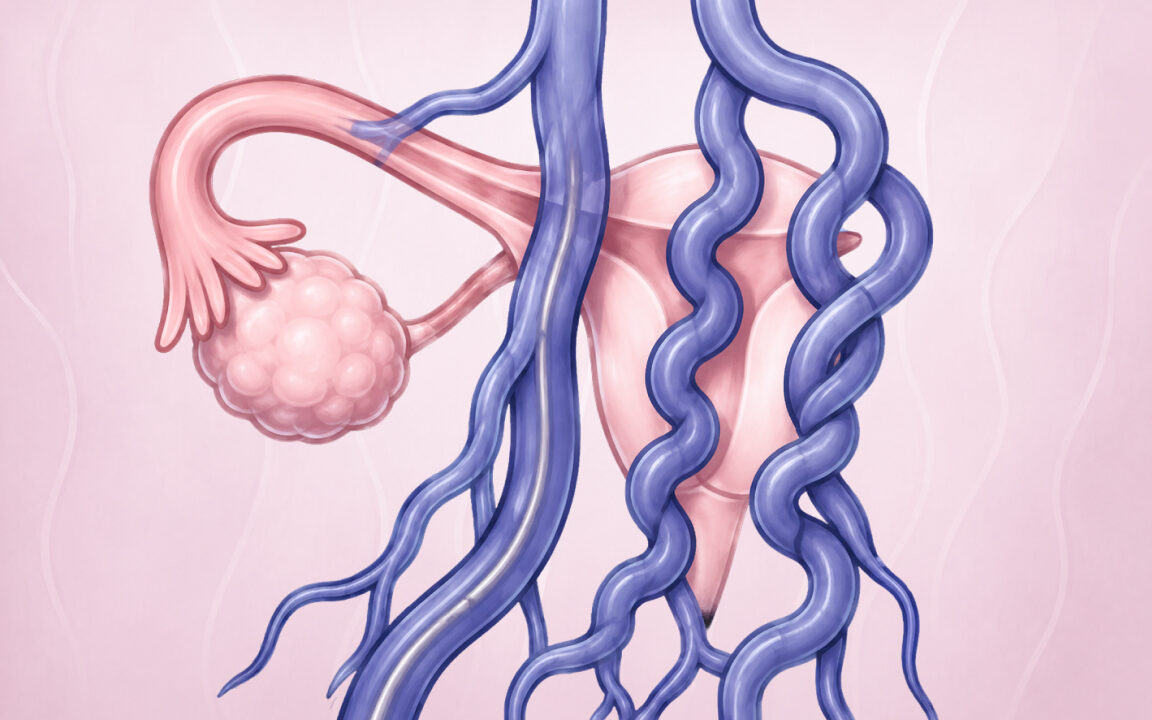










Your pelvic veins have a job.
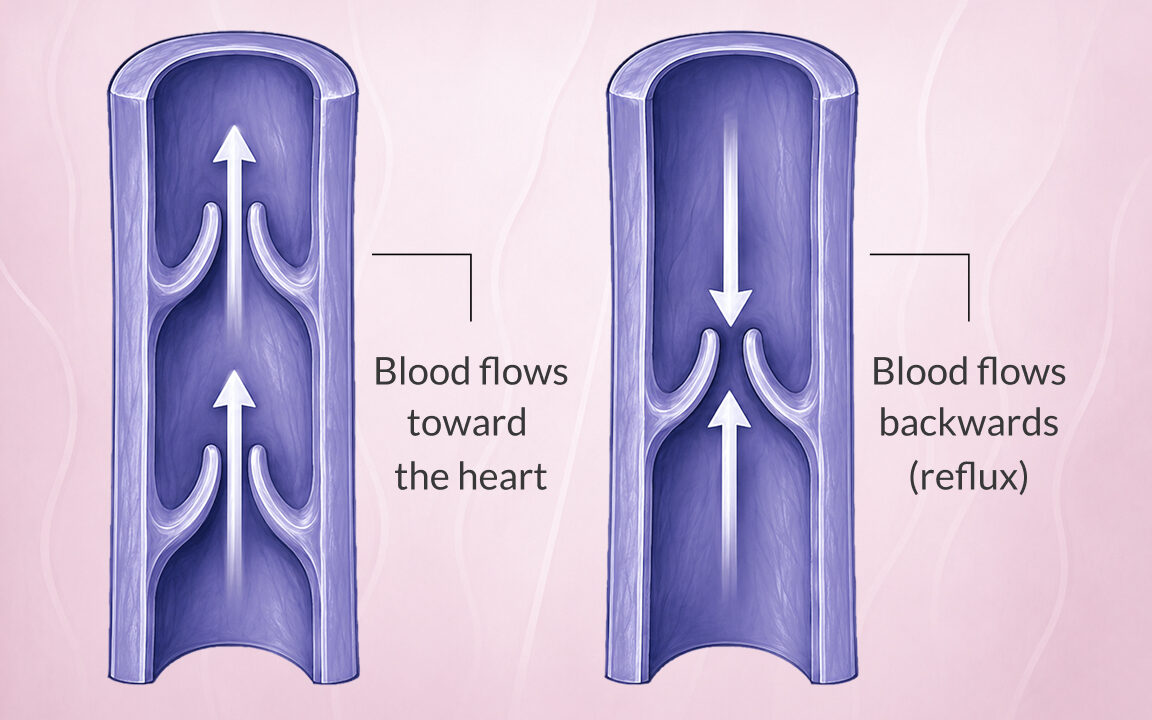
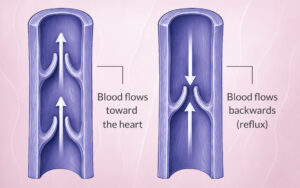
They drain venous blood away from the uterus, ovaries, and surrounding pelvic structures back toward the heart. Inside these veins, small one-way valves prevent blood from flowing backwards. When these valves become incompetent (meaning they no longer close properly), blood begins to flow in the wrong direction. This is called retrograde flow, or reflux.