Many gynaecological and urological conditions share overlapping symptoms with PeVD. Endometriosis, uterine fibroids, ovarian cysts, interstitial cystitis, and musculoskeletal pelvic floor dysfunction can all produce chronic pelvic discomfort. Before embolisation is considered, these conditions must be assessed and either excluded or identified as co-existing factors.
Dr Sriram Narayanan, MBBS, MS (Surgery), FRCS (Glasgow), FRCS (Gen Surg), Dip Lap Surgery (France) — a Senior Consultant Vascular and Endovascular Surgeon practising at Gleneagles Hospital and Mount Elizabeth Novena Hospital — leads The Venus Clinic team with a comprehensive approach that addresses both the medical and psychosocial dimensions of pelvic venous disorder. His evaluation protocol integrates pelvic floor assessments alongside vascular imaging to ensure the full clinical picture is understood before any procedural decision is made. Dr Narayanan brings over two decades of vascular and endovascular surgical experience across the United Kingdom and Singapore to every patient assessment.
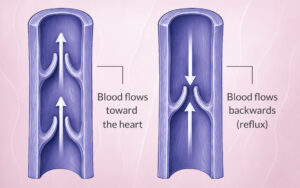
Definitive candidacy requires specialist imaging. Specialist imaging is required to confirm the presence and pattern of pelvic venous reflux before proceeding. Duplex ultrasound is commonly used as an initial screening tool, while cross-sectional venous imaging (CT or MR venography) and diagnostic venography provide more definitive anatomical detail, with catheter-directed venography considered the gold standard for diagnosis and often performed immediately prior to treatment.